













 19 / 34
19 / 34

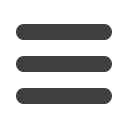
“The tent experience was a very unique and intimate one,” remembers Chris
Addis. M.D., an Internal Medicine Hospitalist from Lancaster, PA. “We spent
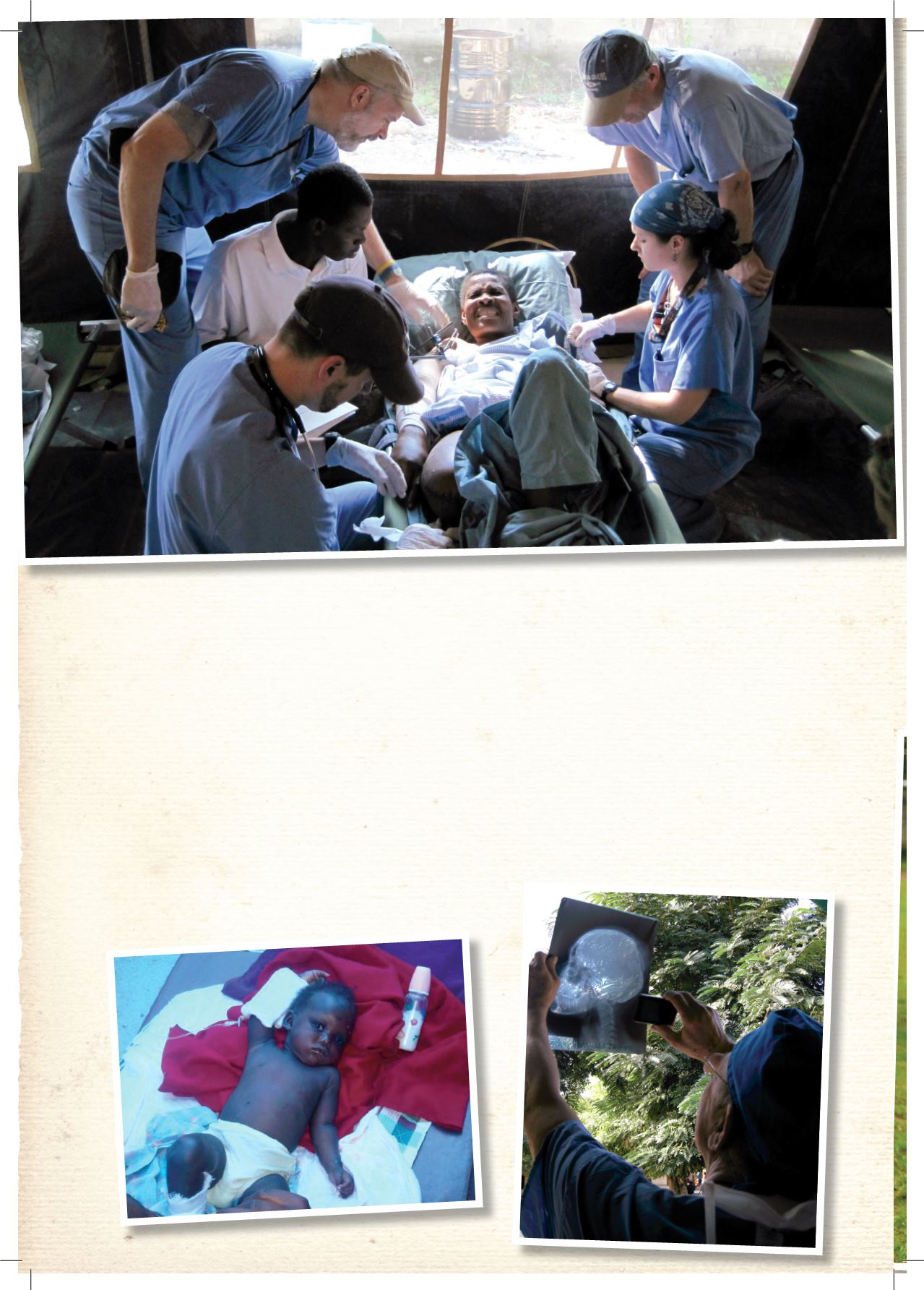
time teaching at the bedside. Our translator obtained a laptop to review DVD-
Radiographs of fractured bones, septic joints, and osteomyelitis. Thus, we were
able to discuss ‘why this patient needs an amputation,’ at the patient’s side.”
Conditions treated ranged from open and closed long bone fractures, deep open
wounds (left untreated for 7-10 days), compression neuropathies from massive
swelling, spinal cord injuries, burns and multiple medical problems. Every wound
was grossly contaminated and severely infected;
several with maggot infestation, ironically
helping to debride (cleanse) the wound.
In the midst of a fast-movingemergency response, those bedside
discussions helped to alleviate patients’ fears and confusion,
encouraging their participation in diff icult clinical decisions.
22